In recent history, fee-for-service (FFS) has been the most popular form of payment. Payors reimburse providers each time that they see a patient and/or for each individual service provided. FFS can incentivize providers to provide as many services as possible and increase prices, which is partly responsible for our expensive healthcare system. Value-based care is when providers get paid for value, which is equal to improved outcomes and reduced cost. VBC theoretically aligns incentives between payers, providers, and patients but has some negative externalities that we discuss below.
Health Systems Transformation to Value
The Case for Vertical Integration in Healthcare
Recently, there has been some skepticism around value-based care, but these troughs and their subsequent peaks are nothing new. The first health plans in the US were “value-based,” in that providers took on financial risk for their patient’s health, acting as a mini-insurer. Dr. Shadid in OKC, Drs. Ross and Loos in LA all started these types of plans in 1929 and were all barred from their local medical societies. In the 1990s, there was significant public backlash against HMOs. Despite this pushback, VBC has curbed health spending by lowering prices, reducing utilization, and incentivizing preventative care. This decrease in spending should not have an effect on overall health, as differences in medical spending generally do not show a statistically significant impact on health outcomes. And what does this reduction in health spending get us? Better education for children, fewer food deserts, and more funding for social safety net programs. At the end of the day, Americans are way too sick, and we are spending way too much on healthcare. It’s not more healthcare that’s going to save us, it’s a healthier lifestyle - one that everyone should have the liberty to access.
“Higher-life-expectancy places didn’t enjoy a greater quantity or quality of medical care, or higher rates of health insurance coverage. Rather, higher-life-expectancy places had populations that smoked less, exercised more, and were less likely to be obese.” - We’ve Got you Covered
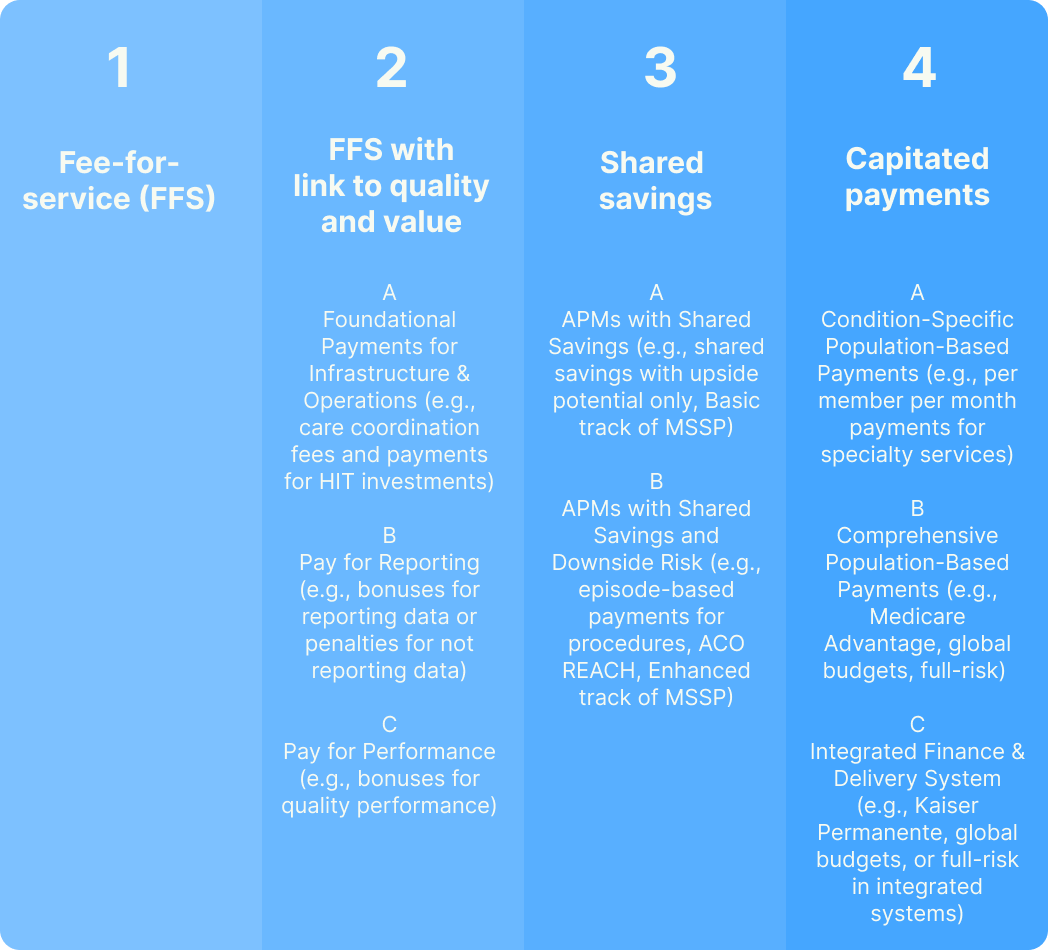
There’s lots of hullabaloo on the definition of VBC (aka Alternative Payment Models (APMs), managed care, accountable care, etc.), so let’s start with the basics. In the US healthcare system, there are 4 primary payment methodologies. While folks in Category 2 like to say they’re doing VBC, in reality, categories 3 and 4 are the real deal and together make up 41.3% of all payments. CMS is hoping to increase this percentage and have 100% of Traditional Medicare beneficiaries in categories 3 and 4 (aka accountable care relationships) by 2030.
Category 1, fee-for-service (FFS): In the FFS model, healthcare providers are reimbursed for each service, test, or procedure they deliver. Each item is assigned a specific fee.
Category 2, fee-for-service with a link to quality and value: A hybrid reimbursement model combining traditional fee-for-service with value-based elements. Providers receive payments based on service volume while also earning more for meeting specific quality and performance metrics. For example, providers can get paid for reducing A1C levels (pay for performance), simply reporting A1C levels (pay for reporting), or adopting an Electronic Health Record (EHR) (foundational payments for infrastructure and operations).
Category 3, shared savings models: The provider organization and the payer establish a prearranged cost benchmark for treating a particular population. If the provider succeeds in delivering care that costs less than this benchmark, the resulting savings are shared between the provider and payer. These payments are often “gated” by quality measures. This methodology is common for Accountable Care Organizations (ACOs) in Traditional Medicare.
Category 4, capitated payments (aka population-based payments): Population-based payments give providers a fixed dollar amount for managing the care of a defined patient population; hence, these providers take on the all of the financial risk for this population. Quality metrics often enhance these payments. Early health plans were aligned to this payment methodology.
In the late 1920s, Dr. Michael Shadid in Oklahoma City and Drs. Paul Ross and Don Loos in Los Angeles pioneered early healthcare payments models that pooled patient resources for prepaid medical care. Dr. Shadid raised money from rural farmers in order to build a hospital and deliver discounted care to invested patients. Meanwhile, the Ross-Loos Medical Group in Los Angeles provided prepaid healthcare to employees of the Los Angeles Department of Water and Power, focusing on prevention and health maintenance. At a time of need (the Great Depression), these efforts stabilized physician income by ensuring a standardized rate, all while aligning incentives toward prevention, as they would pay for poor outcomes and unnecessary treatments. As with many innovations, these efforts faced significant backlash from the medical establishment, particularly the American Medical Association (AMA) and local medical societies, who felt these prepaid models threatened physicians' income and autonomy by introducing fixed payments and administrative oversight. For these reasons, Drs. Shadid, Ross, and Loos were all kicked out of their local medical societies, although Dr. Shadid got redemption in an antisuit suit some 20 years later.
In the 1970-90s, the rise of Health Maintenance Organizations (HMOs) re-introduced a version of prepaid medical groups with federal support. After the introduction of Medicare and Medicaid in 1965, skyrocketing health costs became unsustainable, and the government had to step in. The HMO Act of 1973, championed by the Nixon administration, provided federal support to expand the HMO model. As HMOs grew in prominence, they encountered backlash similar to that faced by the early pioneers. Physicians felt that HMOs prioritized cost savings over patient care, restricting their autonomy with rigid regulations, referrals, and prior authorizations. Patients also criticized HMOs for limited provider networks and denials for certain treatments, leading to a public perception that profit-driven motives compromised the quality of care. In our current iteration of VBC, we have seen quality measures combat the rationing of care and consumer choice promote open networks.
Disclaimer: I got lots of love for all doctors. I don’t mean to be accusatory - just want to acknowledge you all as rational actors in a financial system.